
KUALA LUMPUR, Jan 28 – A new cost-benefit analysis found that capping drug prices in Malaysia may cause more harm than good, severely affecting the economy, the private health care sector, patients, and the country’s access to new innovative treatments.
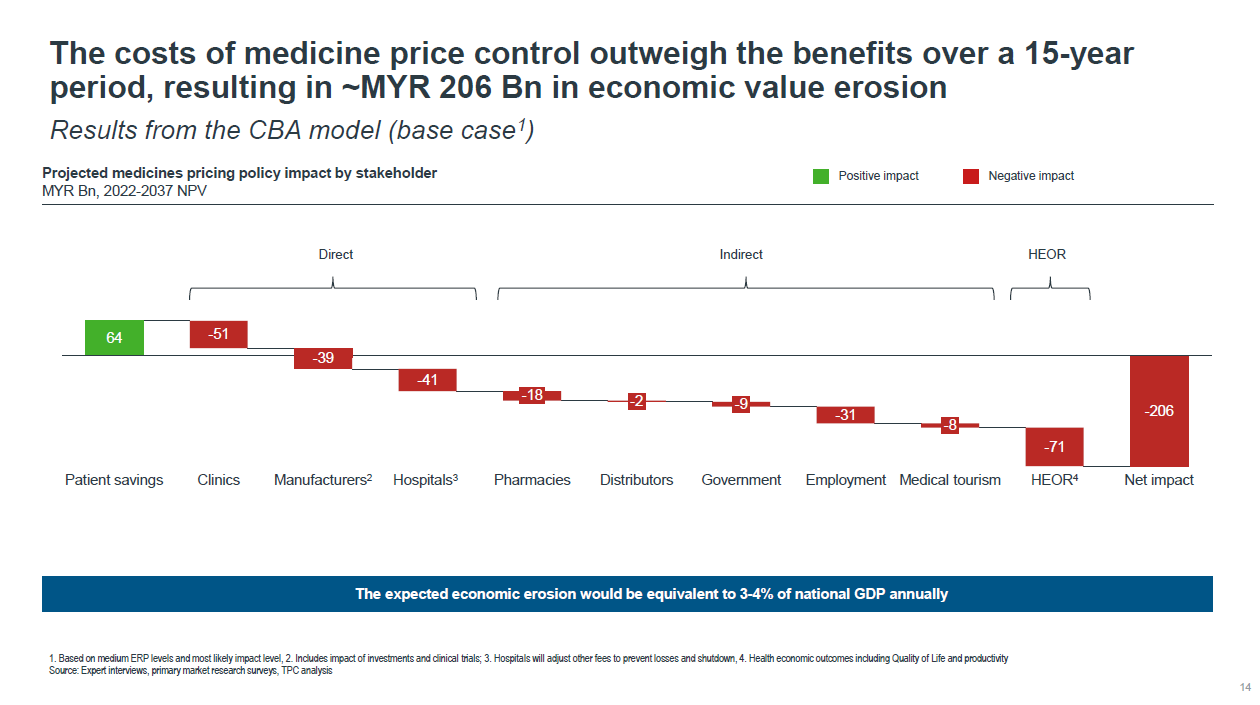
Price controls for medicines could result in a RM206 billion economic value erosion — or overall loss from the private health care sector in Malaysia — over the next 15 years from 2022 to 2037.
This is equivalent to 3 to 4 per cent of Malaysia’s national gross domestic product (GDP) annually, according to the “Comprehensive Cost-Benefit Assessment on the Medicine Pricing Policy (Preliminary Findings)” public consultation document by the Malaysia Productivity Corporation (MPC), as sighted by CodeBlue.
“The medicine price control will severely impact PHC’s (private health care) stability as a sector and result in overall loss of MYR 206 Bn, decreased access and poorer health outcomes for Malaysian rakyat,” said the cost-benefit analysis report, noting that at status quo, the private health care sector will generate RM1 trillion over the next 15 years.
This assessment, based on a public consultation session with private industry groups from November 29 to December 6 last year, was commissioned by the government to review the wider economic impact of the Ministry of Health’s (MOH) proposed medicine price controls on the private health care ecosystem and people’s health, as well as the impact on the overall economy and aspects of the Malaysian government.
MOH wants to regulate medicine prices in the private health care sector by using an external reference pricing mechanism to cap wholesale prices and subsequently set retail ceiling prices of prescription drugs in private hospitals, clinics, and pharmacies, based on regressive markups from the wholesale ceiling price. External reference pricing is determined by comparisons of drug prices in Commonwealth countries, other countries in the region, or those with similar income levels as Malaysia.
While MOH’s proposed drug price control policy could save patients RM64 billion in medicine bill and insurance premium savings over the 15-year period at net present value, its overall impact, including on hospitals, pharmacies, and employment, would be negative, the latest cost-benefit analysis found.
Net present value (NPV) or net present worth is a method used to determine the current value of all future cash flows generated by a project or investment. It is used to calculate today’s value of a future stream of payments.
The preliminary findings of the cost-benefit analysis found that the overall cost-to-benefit ratio is about 4.3:1, meaning that for every RM1 saved, around RM4.30 is lost to Malaysia.
“Hence, we recommend the Malaysia government to re-evaluate alternative options to medicine price control or mitigating solutions to reduce medicine price control impact,” concluded the cost-benefit assessment.
The cost-benefit analysis suggested that while medicine price controls could result in a 1 per cent to 14 per cent increase in patients in the private health care sector, about 90 per cent of the expansion would come from the middle 40 per cent (M40) and top 20 per cent (T20) income groups, with the bottom 40 per cent (B40) least likely to benefit.
The policy could see 2,600 private clinics shut down, especially smaller clinics, resulting in reduced health care access or an economic value loss of RM51 billion at NPV.
In the short term, private hospitals are expected to close their outpatient services to stay afloat. In the long run, they may consider leaving the Malaysian market, which would result in a further economic value loss of RM41 billion.
Pharmacies and distributors will also be impacted, albeit to a lesser extent, further disrupting access along the health care supply chain. This, the report estimated, could lead to a combined economic loss of RM20 billion at NPV over the 15-year period from 2022 to 2037.
Critically, pharmaceutical manufacturers may withdraw current innovative therapies and delay new innovative drug launches, while generic drugs may be diverted for export, which could cause a massive loss of RM51 billion. As a result, poorer health outcomes will be borne by the Malaysian people.
From the economic perspective, it is estimated that between 91,000 and 136,000 jobs and salaries in the private health care sector will be impacted, while the government could also see reduced income from tax, investment (loss of RM9 billion), and medical tourism (NPV loss of RM10 billion).
Medical tourism is expected to decline despite 7 per cent growth in volume, resulting in NPV loss of about RM8 billion to the economy, as Malaysia will likely be deprioritised and become less attractive for pharmaceutical companies to launch new drugs.
The analysis stated that the decrease in tax revenue for the government may impact its fiscal balance, currently at -6.2 per cent, and the country’s GDP growth target of 4.5 per cent to 5.5 per cent per annum as per the Twelfth Malaysia Plan (12MP).
“Despite its good intentions, the policy will not likely achieve much improved health care access, rather, it could have detrimental effects on Malaysia’s economy,” the report concluded.
The Comprehensive Cost-Benefit Assessment (CBA 2.0) on the medicine pricing policy is the second cost-benefit analysis of proposed drug price controls. It covers about 5,000 products, expanding the product scope beyond the first cost-benefit analysis, with MPC describing this latest review as a “more holistic impact assessment” of proposed drug price controls through “data-driven insights”.
MPC served as the lead government coordinating body that coordinated and facilitated the public-private collaboration on the CBA between government agencies, independent economists, and groups representing local and foreign pharmaceutical manufacturers, multinational pharmaceutical companies, private hospitals, and medical doctors.
The CBA 2.0 working group comprises five members from the private health care industry: the Pharmaceutical Association of Malaysia (PhAMA); the Malaysian Organisation of Pharmaceutical Industries (MOPI); the Association of Private Hospitals, Malaysia (APHM); the Malaysian Medical Association (MMA), and the Pharmaceutical Research & Manufacturers of America (PhRMA).
Members of the CBA 2.0 working group among government bodies include the Ministry of International Trade and Industry (MITI), MOH, the Ministry of Finance (MOF), Bank Negara Malaysia (BNM), the Economic Planning Unit (EPU), the Malaysia Healthcare Travel Council (MHTC), the Intellectual Property Corporation of Malaysia (MyIPO), the Department of Statistics Malaysia (DOSM), and MPC.
The academicians who are part of the CBA 2.0 working group comprise Emeritus Professor Zakariah Abdul Rashid, Prof Kenneth Kwing Chin Lee from Monash University Malaysia, and Nur Ain Shahrier from Sunway University Malaysia.
The cost-benefit analysis was undertaken by an appointed independent global data science company that MPC did not name.
This is the first part in a series of stories on the “Comprehensive Cost-Benefit Assessment on the Medicine Pricing Policy (Preliminary Findings)” document by the Malaysia Productivity Corporation on its public consultation from November 29 to December 6, 2021.
- Part Two: Medicine Price Controls: Clinic Closures, RM31Bil Wage Loss In Private Health Care
- Part Three: Medicine Price Controls Benefit Rich The Most, Poor The Least
- Part Four: Drug Price Controls May Slash 60% Of Medical Tourism Revenue
- Part Five: Medicine Price Controls Risk Malaysia Losing Innovative Drug Launches





