
KUALA LUMPUR, Feb 2 – Proposed price controls for prescription drugs will not significantly expand private health care access for the low-income, with the richest expected to benefit the most instead.
A cost-benefit analysis on the proposed policy, published by the Malaysia Productivity Corporation (MPC) and sighted by CodeBlue recently, showed that while drug price controls will result in significant savings of up to 50 per cent for patients seeking medical service in private clinics, the price difference is lower in hospitals at 20 to 25 per cent.
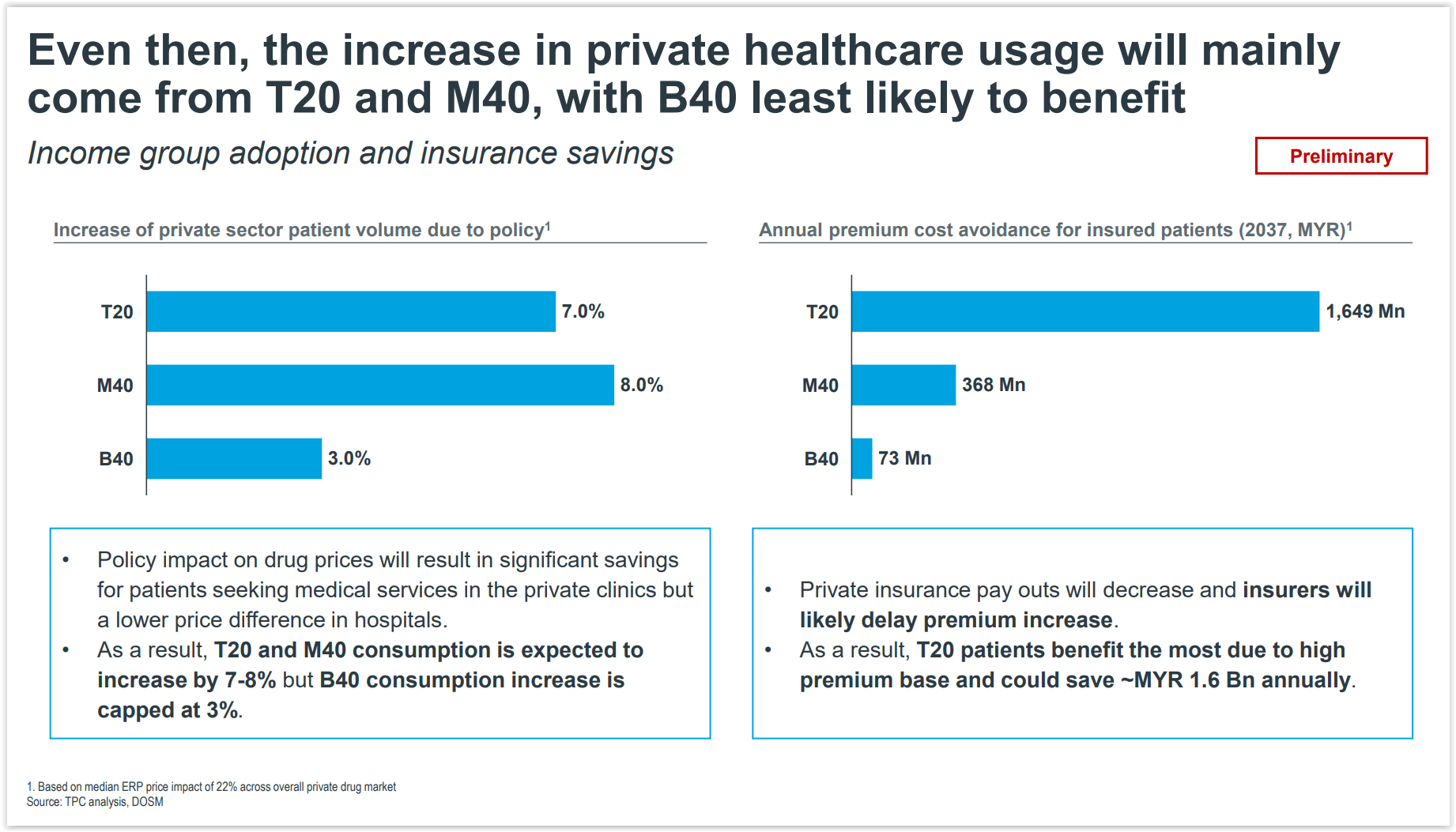
As a result, private health care consumption by the top 20 per cent (T20) and middle 40 per cent (M40) income groups is expected to increase by 7 to 8 per cent, but the bottom 40 per cent (B40) income group’s consumption increase is capped at 3 per cent.
Private insurance payouts will also decrease and insurers will likely delay raising premiums. In turn, this will benefit T20 patients the most due to their high premium base.
Preliminary findings of the cost-benefit study project that insured T20 patients could save up to RM1.6 billion annually over a period of 15 years from 2022 to 2037, versus annual savings of RM368 million by M40 patients and RM73 million by B40 patients.
The Comprehensive Cost-Benefit Assessment (CBA 2.0) on the medicine pricing policy conducted with private industry groups from November 29 to December 6 last year is the second cost-benefit analysis of proposed drug price controls.
It covers about 5,000 products, expanding the product scope beyond the first cost-benefit analysis, with MPC describing this latest review as a “more holistic impact assessment” of proposed drug price controls through “data-driven insights”.
Former Health Minister Dr Adham Baba previously said that the then-Perikatan Nasional government would implement price controls on medicines through the Price Control and Anti-Profiteering Act 2011 (Act 723), as mooted by the Pakatan Harapan administration.
He said the measure would be executed in the public and private sectors to ensure that treatment costs in private hospitals do not increase arbitrarily.
Dr Adham said the wholesale ceiling price for medicines would be determined based on the External Reference Price (ERP), a price comparison with Commonwealth countries, regional countries, and countries that have close gross domestic product (GDP) used as benchmarks in negotiations.
Retail ceiling prices of prescription drugs in private hospitals, clinics, and pharmacies would then be set based on regressive markups from the wholesale ceiling price.
This is to ensure that the price of medicines in Malaysia is equivalent to other upper middle income countries and does not exceed prices in high-income countries.
This is the third part in a series of stories on the “Comprehensive Cost-Benefit Assessment on the Medicine Pricing Policy (Preliminary Findings)” document by the Malaysia Productivity Corporation on its public consultation from November 29 to December 6, 2021.
- Part One: Medicine Price Controls May Erase RM206Bil From Economy
- Part Two: Medicine Price Controls: Clinic Closures, RM31Bil Wage Loss In Private Health Care
- Part Four: Drug Price Controls May Slash 60% Of Medical Tourism Revenue
- Part Five: Medicine Price Controls Risk Malaysia Losing Innovative Drug Launches




