
KUALA LUMPUR, March 1 — Malaysia has already passed the containment phase of the Covid-19 epidemic and entered mitigation, as there is widespread community transmission of the virus, public health expert Dr Lokman Hakim Sulaiman said.
Hence, the objective of mitigation is no longer to completely control transmission of the coronavirus, a containment strategy, but to ensure that the health care system is not under pressure and to protect people from developing severe disease or dying from Covid-19.
“Therefore, to only test symptomatic people is appropriate in the mitigation phase,” Dr Lokman wrote on Facebook yesterday.
“However, what is not appropriate, or a peculiarity, is the continued use of containment interventions, like the MCO (Movement Control Order) or PKP (Perintah Kawalan Pergerakan), during the mitigation phase.
“What is needed is to ensure that people with symptoms are confirmed to be infected with Covid-19 within 24 to 48 hours from the start of symptoms. For that, access to antigen RTK tests must be widened.”
Dr Lokman, who is a professor of public health at the International Medical University (IMU) and former Health deputy director-general (public health), stressed that entering the mitigation phase of the coronavirus epidemic was “not a failure”.
“This is the normal cycle in the management of any disease outbreak. This ‘old school of thought’ in conventional epidemiology and outbreak management is still relevant till today,” added the public health expert.

As Malaysia has already entered the mitigation phase of the epidemic, said Dr Lokman, the government must end the MCO and lift interstate or inter-district travel restrictions. He pointed out that the Klang Valley MCO had no impact whatsoever on the coronavirus epidemic in Pahang, Kelantan, and Terengganu that experienced a continuous rise in cases since before the second nationwide lockdown.
“To me, it is not the MCO or PKP 2.0 now that determines success in managing Covid-19. Please accept the fact that this infection cannot be eliminated without total lockdown for at least six months, which will also kill the economy and livelihood,” said the IMU pro-vice chancellor (research).
“We must learn to live with this virus,” he added, citing non-pharmaceutical measures like testing, wearing face masks, and avoiding indoor social gatherings.
The government previously extended the MCO in Selangor, Kuala Lumpur, Johor, and Penang until March 4, while other states were put under the Conditional Movement Control Order, except for Perlis under the Recovery Movement Control Order. There appears to be no discernible difference between the various lockdown measures, as interstate and inter-district travel restrictions are in effect nationwide.
The Ministry of Health (MOH) has never formally declared that Malaysia has already entered the mitigation phase of the Covid-19 epidemic, even though more than 300,000 total coronavirus cases were reported as of yesterday, infecting nearly 1 per cent of the population. Malaysia took 11 months to record the first 100,000 Covid-19 cases on Christmas Eve, but just one month to record the next 100,000 infections by end January, and another month for the third 100,000 cases.
Instead, the government repeatedly harps on “breaking the chain of transmission”, with Health director-general Dr Noor Hisham Abdullah claiming that Covid-19 cases could be reduced to 1,000 a day by mid-March and to below 100 daily by May. Malaysia’s reported coronavirus cases dropped from about 5,000 at the end of January to about 2,500 at the end of February, based on five-day moving averages.
He made his projection based on public health measures and the national Covid-19 vaccination programme, even though the first phase of the inoculation drive only targets frontliners: mostly health care workers and law enforcement. Most coronavirus clusters have been reported from workplaces, including factories, not among frontline health care providers. It is unclear when workers, including migrant workers, can get vaccinated.

Dr Lokman disputed the official narrative that the reported reduction of daily Covid-19 cases was due to the MCO 2.0 enforced since January 13.
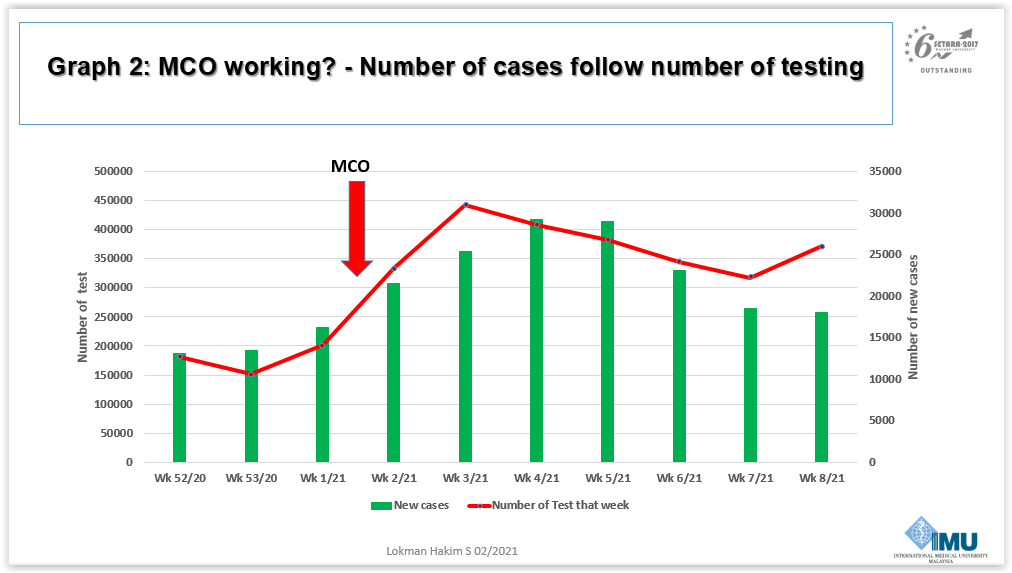
“In my opinion, this is an epidemiological artifact,” he said. “The number of reported cases follows the trend of testing of samples. The more you test, the more cases will be reported. When the number of samples tested decreases, the number of cases also declines.”
Dr Lokman linked the reduced testing to MOH’s change of policy last January from screening all close contacts of positive Covid-19 cases to only testing those with symptoms. On February 17, after some public criticism, Dr Noor Hisham retracted MOH’s policy excluding asymptomatic people from testing and said in an internal circular that all close contacts would be tested.

The decline in the number of samples tested, Dr Lokman said, caused Malaysia’s positive rate (share of tests that are positive) to exceed the World Health Organization’s (WHO) 5 per cent benchmark since late last year. WHO said in May last year that a positive rate below 5 per cent for at least two weeks is one indicator that the Covid-19 epidemic is under control in a country.
Dr Lokman also noted an apparent ramp-up in Covid-19 testing in Malaysia from the first week of this year, but a subsequent decline from the third week of 2021.
“This is very different from MCO or PKP 1.0, when the positive rate was extremely low at below 5 per cent, indicating aggressive action in testing as many people as possible to detect as many cases as possible. Because of that, we succeeded well in flattening the epidemiological curve during MCO or PKP 1.0,” he said, referring to Malaysia’s first strict seven-week lockdown from March last year.

The public health expert expressed concern that limited access to antigen RTK testing would prevent symptomatic people from getting diagnosed with Covid-19 and, thus, lead to high risk of death for vulnerable groups.
He observed a rise in weekly deaths from Covid-19 in Malaysia since the past four months, exceeding 100 each in the fifth and sixth epidemiological weeks of 2021.

RM70 for antigen RTK in the private sector, Dr Lokman said, was too expensive. MOH criteria for free testing on symptomatic people, according to patients-under-investigation and close contact definition, were too restrictive, despite a high number of sporadic infections in the community.
He called for antigen RTK to be expanded to all public health clinics with medical assistants and nurses, saying that these staff can be trained to do such testing in any space with good ventilation. MOH’s requirement of special safety cabinets at clinics for antigen RTK, said Dr Lokman, is not mandated by WHO that only moots the point-of-care testing to be done in well ventilated spaces with appropriate protective gear.
“RTK should be done for free or at a subsidised rate, including in private facilities, so that people are not prevented from getting tested. The SOP and diagnostic criteria must be amended immediately, according to mitigation principles and testing objectives.”





