

The bulk and thrust of the concerns of the signatories (Concerned Malaysian Medical Practitioners) of the letter to the prime minister, health minister, and the National Security Council address the association of the Covid-19 mRNA vaccines with the risk of acute myocarditis (point numbers 7 to 15).
This brief, a summary of relevant review articles, will examine the evidence, notably the risk benefit analysis, related to their concerns and allegations, and demonstrate that their allegations are unfounded and their concerns totally misplaced.
Acute myocarditis is often associated with a viral infection, and the SARS-CoV-2 is no exception. Prior to the advent of Covid-19, the estimated incidence of viral myocarditis was 10-22 cases per 100,000 persons.
The largest population study to date of acute cardiac outcomes estimated an extra 40 myocarditis events per one million due to SARS-CoV-2.
This is at least four to 40 times higher than mRNA vaccine-associated myocarditis, which is estimated at one to 10 per one million vaccinated persons in multiple studies. (Klein, N. P. et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA 326, 1390–1399, Montgomery, J. et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US Military. JAMA Cardiol. 6, 1202–1206).
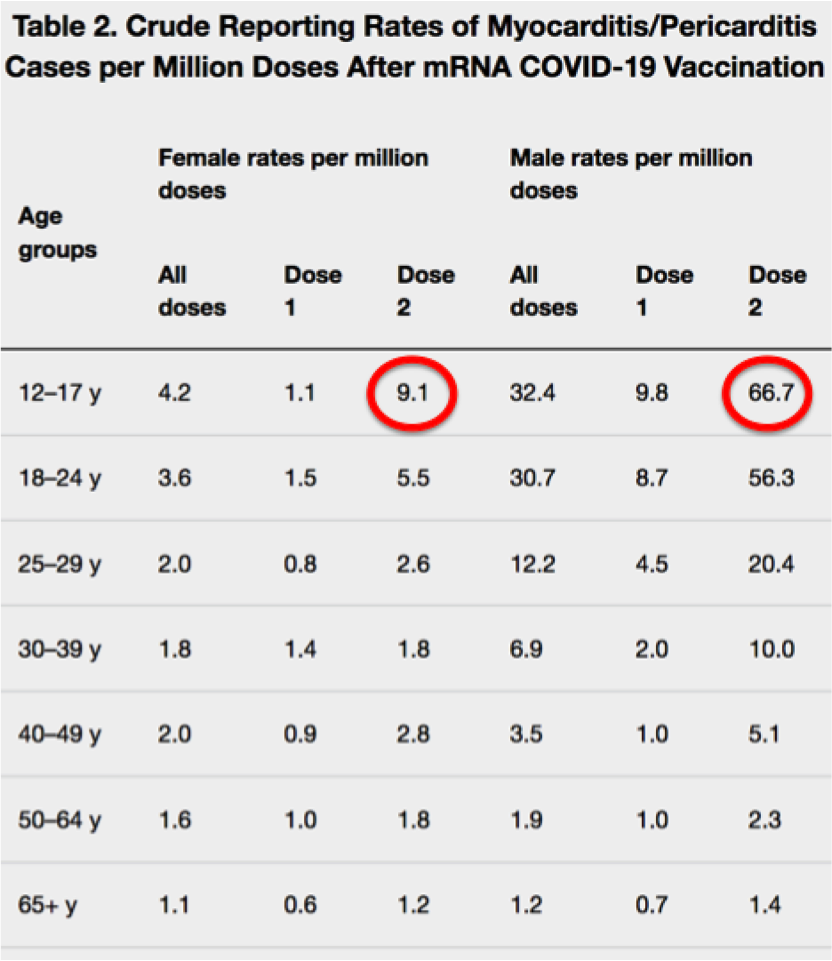
As in post-viral myocarditis, mRNA vaccine associated myocarditis occurs mainly in young males under 20, and usually after the second mRNA vaccine dose. The estimated reported rates was 67 per million. The majority of the cases were present within one week of the mRNA vaccination.
In young males, myocarditis due to Covid-19 was estimated to occur at a rate as high as 450 per million. Therefore, young males infected with SARS-CoV-2 are at least six times more likely to develop myocarditis compared to those who have received the mRNA vaccine.
With the upcoming immunisation for children aged 5 to 11, parents should be further reassured that the risk of post-mRNA vaccine myocarditis is remarkably low. Only 11 cases were reported from a total of 8.7 million doses and all have virtually recovered.
Overall, the clinical course of post mRNA vaccine-associated myocarditis is mild, and the outcome is very good, with a survival rate in excess of 99 per cent. More than 90 per cent of the patients recover their cardiac function within a few weeks of the injury.
In contrast, Covid-19 associated myocarditis runs a much higher risk of cardiac injury. 10 per cent of Covid-19 outpatients and 40 per cent of inpatients have significant cardiac complications in the absence of coronary artery disease.
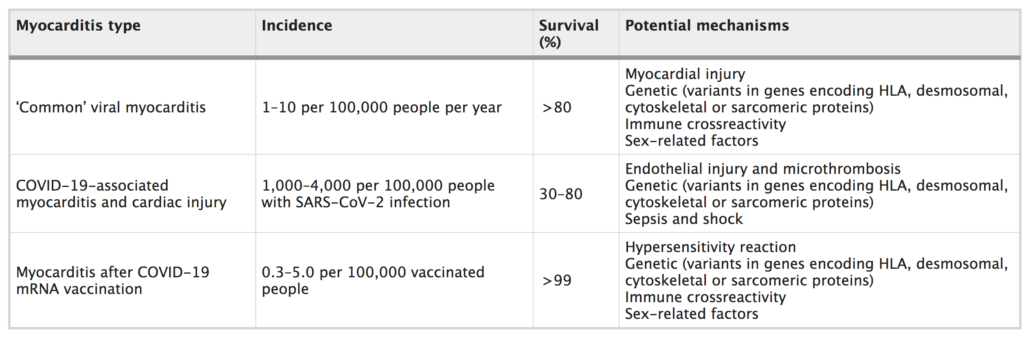
The low oxygen, shock syndrome, blood clots, bleeding and vessel injury seen in patients with Covid-19 further compound the myocardial damage. The survival rate following Covid-19 associated myocarditis is much lower, between 30 and 80 per cent. (Aikawa, T., Takagi, H., Ishikawa, K. & Kuno, T. Myocardial injury characterized by elevated cardiac troponin and in-hospital mortality of COVID-19: an insight from a meta-analysis. J. Med. Virol. 93, 51–55).
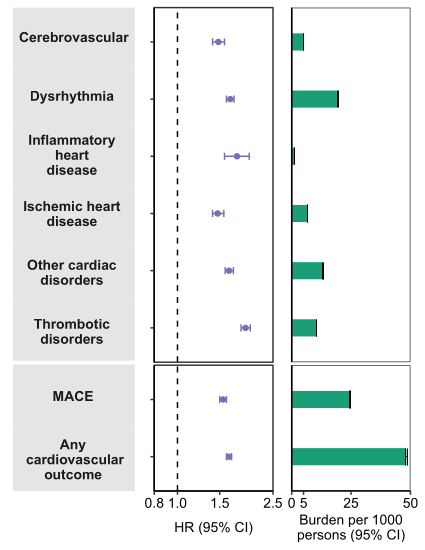
And while we are still discussing the acute conditions of the heart, we would like to draw attention to a whole series of chronic cardiac injury and complications related to long Covid.
Over the course of a one-year follow-up, Covid-19 survivors showed a significantly increased risk and burden of cerebrovascular disorders, dysrhythmias, inflammatory heart disease, ischemic heart disease, heart failure, thromboembolic disease, and other cardiac disorders.
Apart from the acute myocarditis which we have earlier described, the Covid-19 pandemic has also caused a significant increase in the global burden of other chronic debilitating cardiovascular diseases. This will further burden already-overwhelmed health care systems worldwide.
We have confined ourselves to the main allegation of the letter, namely the lack of safety of mRNA vaccines and its causation of acute myocarditis.
We are sure other colleagues and professiona; medical organisations will address the other preposterous allegations and anti-vaccine nuances of the aforementioned letter.
The letter is very reminiscent of Wakefield’s withdrawn publication in The Lancet regarding Measles-Mumps-Rubella (MMR) vaccines and autism. We must follow the science, and not present data in snippets to further advocate an extremely dangerous and malicious agenda.
We have shared incontrovertible evidence which debunks their allegations, and we would like to advocate the continuing use of mRNA vaccines to mitigate Covid-19 cases, hospitalisations, ICU admissions, deaths, and to help us exit from the pandemic.
From a public health perspective, vaccines serve as the best protection against new and emerging variants, especially with the opening of schools and public spaces, and the implementation of the National Recovery Plan 2.0, whereby border restrictions will be eased.
Since the number of Covid-19 paediatric cases are rising in the United States and Europe, we must take heed and encourage vaccinations for the vulnerable segments of the population.
In summary:
- Myocarditis cases following mRNA vaccination are rare.
- Myocarditis cases due to Covid-19 are very much higher than cases of myocarditis following mRNA vaccinations.
- Cases of mRNA vaccine-associated myocarditis are mild, and the outcome is good.
- Cases of myocarditis due to Covid-19 are associated with a higher risk of myocardial injury, complications, and death.
- Evidence-based risk benefit assessments show that mRNA vaccinations are overwhelmingly preferable to acquiring Covid-19 associated myocarditis, and should continue to be recommended.
- Cardiovascular diseases associated with long Covid can be mitigated with increased and better utilisation of mRNA vaccines.
Dr Musa Mohd Nordin is a paediatrician, Dr Zulkifli Ismail is a paediatric cardiologist, and Asst Prof Mohammad Farhan Rusli is a public health physician.
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.

