
Since the Ministry of Health (MOH) has embargoed all Covid-19 data, it is virtually impossible to decipher their rationale for extending this next round of the Conditional Movement Control Order (CMCO) from 9 Nov – 6 Dec 2020.
What is the matrix the National Security Council (NSC) or MOH is using to impose another round of CMCO? We searched high and low for the science mandating an extension of the CMCO but it is not forthcoming from either the NSC or the MOH.
With the assistance from our Public Health (PH) and Infectious Diseases (ID) physician colleagues, we would like to offer data and trends captured from MOH’s statistics in the public domain that makes the CMCO untenable from the perspectives of Evidence Based Medicine (EBM).
Absolute numbers of Covid-19 cases in any one state is not a useful parameter for the sake of comparison between states. It needs to be expressed as a proportion of the state’s population. This is a basic statistical tool for meaningful comparison.
Figure 1 courtesy of Prof Datuk Dr Lokman Hakim, illustrates the Incidence Rate (per 100,000 population) plotted from the epidemiology weeks 40 till 44 weeks (1st week of October until 1st week of November 2020).

Eyeballing the graph, one can immediately summarise that the two problem states which merits the consideration of an MCO are Labuan and Sabah. The Incidence Rates in KL, Melaka, Sarawak, Pahang, Johor, Perak, Perlis, Terengganu and Kelantan are virtually negligible in comparison. And the upticks in the Incidence Rate in Putrajaya, Negeri Sembilan, Kedah, Selangor and Pulau Pinang can be best managed with a robust Test-Trace-Isolate-Support (TTIS) response without the imposition of a nationwide CMCO.
The MCOs are inflicting devastating damage on individual, family, community and national economic activity, impacting severely on our daily livelihoods, driving families and communities to below the poverty line.
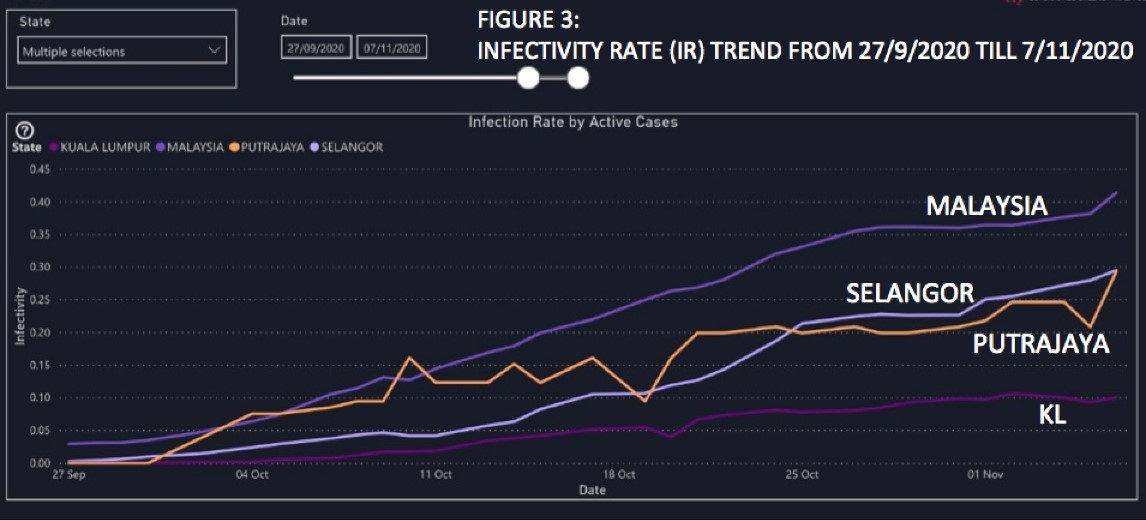
The Infectivity Rate (IR) by state is the number of active Covid-19 cases per 1,000 population.
Figure 2 (Yellow Bar Graph of Active Cases) represents the latest IR that was calculated on 6 November 2020 when the population numbers were taken into account.

The immediate observation is that the IR (in brackets) in the territories of the Klang Valley, Selangor (0.295), Putrajaya (0.294) and KL (0.101) are well below the national average of 0.414 under the current CMCO. It is misleading to look at any one point in time (date specific) to make a comparison of their respective performances. Instead, we should look at the trends of IR to arrive at any valid scientific conclusions.

Figure 3 (Line Graph) represents the trend of IRs beginning from 27/09/2020 (just before the start of CMCO 2.0 on 14.10/2020) till 7 November 2020, which reaffirms that the IR trend for all the three territories in the Klang Valley are well below the national average.
If anything, the IR trend for KL, the hub of the nation’s economic activity is flattening and a continuation of CMCO does not make any scientific nor economic sense.
Even the IR trends in both Selangor and Putrajya are decelerating compared to the period of 11-25 October, except for the most recent uptick in Putrajaya.
Therefore, it is difficult to comprehend the assertion that “the decision to order a partial lockdown in six peninsular states came about because conditional movement control orders (CMCO) take time to have effect.”
Another commonly cited metric is the Reproduction Number (RO) or it’s sister RT where it is being used now. RT (or a compartmentalization model of RO) is inherently complex, from which no independent review can be made unless the author discloses the many assumptions that has been made.
The complexity of RT, combined with its tendency to be skewed by the on-the-ground context (for e.g. a new big cluster in a detention centre in District A which is isolated from the community of District A), contributes to the lack of a systematic and daily reporting by MOH of the RT figure for each state.
This sporadic and inconsistent manner of RT reporting compels us to question the reliability of the MOH’s use of the RT as a metric to determine the start or end of an MCO.
To muddy the situation further, in an earlier article, we have discussed the limitations of the R0 within the context of the new science of the super-spreader phenomenon of the coronavirus and the more exact value and usefulness of the new variable, the dispersion factor “k”.
Notwithstanding, in the same media report (FMT 7/11/2020), the MOH stated that: “If we look at the start of the third wave, the infection rate (R0) was at 2.2 but in two weeks we have brought it down from 1.5 to 1.0.”
From Prof Datuk Dr Lokman Hakim’s Incidence Rate and our IR figures, the infection rate has somewhat plateaued in KL and is decelerating and improving in both Selangor and Putrajaya. And if we are to accept face value the MOH’s R0 figures, the transmission rate has been decreasing to virtually normal at 1.0.
The sensible and scientific decision would be to lift the CMCO, not to prolong it further.
As we alluded in our earlier article, the end-game of any degree of physical distancing, in our case the MCO, is to quickly suppress the total positive cases, reduce the case fatality rates (CFR), provide immediate relief to the health care system and to allow the infected, isolated and quarantined healthcare workers (HCW) to stay alive, get better and get back to work. It buys precious time, such that the health care capacity is protected and not overwhelmed.
All the data currently at our disposal suggest that the MOH was on top of the Covid-19 situation in the Semenanjung, and that health care facilities were neither threatened nor overwhelmed.
At no point in time was the health care capacity in the Semenanjung challenged nor compromised, unlike the criticality of health care facilities in Sabah.
These scientific rationale among others, debunks the need for any form, nor any further continuation of the MCO.
But the critical proviso is that, the built in Testing-Tracing-Isolation-Support (TTIS) rapid response must be functional and robust.
For surveillance purposes, we strongly recommend the mass utilisation of the RTK-Ag instead of the RT-PCR for reasons which are now universally accepted namely, it’s rapid Turn Around Time (TAT), simplicity of use, cheap and can be widely used at the Point of Care (POC).
The World Health Organization (WHO) and its multiple partners are making the rapid test antigen kits available at USD5 per kit to all Low and Middle Income Countries (LMIC), including Malaysia, which is at least 15 times cheaper than the PCR. This is definitely the SARS-CoV-2 detection test of choice in the field, given it’s accuracy as a test of contagiousness of the coronavirus and the difficult economic times we are going through.
We appeal to the NSC to make this test available in the both the public and private health sectors at an affordable price, so that now everyone can test. Like face-masks and PCR, previously, early in the epidemic, the prices of RTK-Ag is astronomical and unaffordable in private laboratories and health facilities.
Prices of RTK-Ag range from RM200-280 per test when the WHO price is USD5 per test. Even if we add in PPEs and labour cost it should not breach RM80-100 per test.
The MOH should benchmark itself against the best in the pandemic crisis management of Covid-19. The following key indicators would determine whether our Test-Trace-Isolate-Support (TTIS) Rapid Response process is robust enough and able to detect cases, trace the contacts and isolate them promptly within 48 hours.
- What percentage of tests are done and results returned within 24 hours?
- What percentage of cases with a positive test are successfully contacted within 24 hours to trace their contacts?
- What percentage of positive cases share their close contacts with the contact tracers?
- What percentage of named contacts are tracked within the next 24 hours?
- What percentage of contacts comply with isolation?
- And, if someone with symptoms has a test that is negative and symptoms persist, how quickly do they receive another test?
It is very critical to emphasise that Malaysia’s Covid-19 strategy must be informed by and adapted to the local context, with the use of evidence-based measures, not blunt outbreak tools.
The CMCO is like a blunt scalpel and any surgeon would know that a blunt scalpel cannot excise a cancer, but would instead inflict unnecessary and collateral damage to the surrounding tissues.
Thus CMCO alone, without a large-scale data-driven testing to detect cases early, swift contact tracing and isolation, would not be sufficient to contain Covid-19. Rather, it may just lead to a longer and longer lockdown, or the nation will be trapped in cycles of lockdowns and openings that will ravage the economy, negatively impact the education of our children, impede access to health care for non-Covid-19 patients and mess terribly with our mental health.
Given the negative repercussions of lockdowns, we must always be ahead of the curve and utilise the right outbreak tools – evidence-based and data-driven – and not rely solely on blunt scalpels. The rakyat and the economy is haemorrhaging.
If the MOH is able to ensure that our Test-Trace-Isolate-Support (TTIS Response) meets the Rapid Response key indicators, then rest assured we can do without more MCOs and can move on with our daily lives within the context of the new normal.
With experience and wisdom gained from the handling of the second wave, we should now be charting an exit strategy and transitioning from MCOs towards a smart and integrated TTIS Response strategy which is critical if we as a nation are to protect the lives of our rakyat, prevent disruptions to our livelihoods, reboot our national economy and secure long term health of our rakyat and the well being of our socio-economic and political life.
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.



