

One of the key preparations before performing the Hajj or umrah is getting the necessary vaccinations. With a large congregation of about two million pilgrims every year, Saudi Arabia’s health ministry keeps a close watch on health requirements to prevent turning the Holy Land into a hotspot of infectious diseases.
Some vaccines are made mandatory before one can perform the Hajj, such as that for invasive meningococcal disease. Others, though not compulsory, are highly recommended by the Saudi health ministry.
The Saudi health ministry publishes annually the health requirements for Hajj in Mecca.
Invasive Meningococcal Disease (IMD)
The Saudi health ministry vaccination requirements for IMD have evolved in response to the changing serogroup epidemiology.
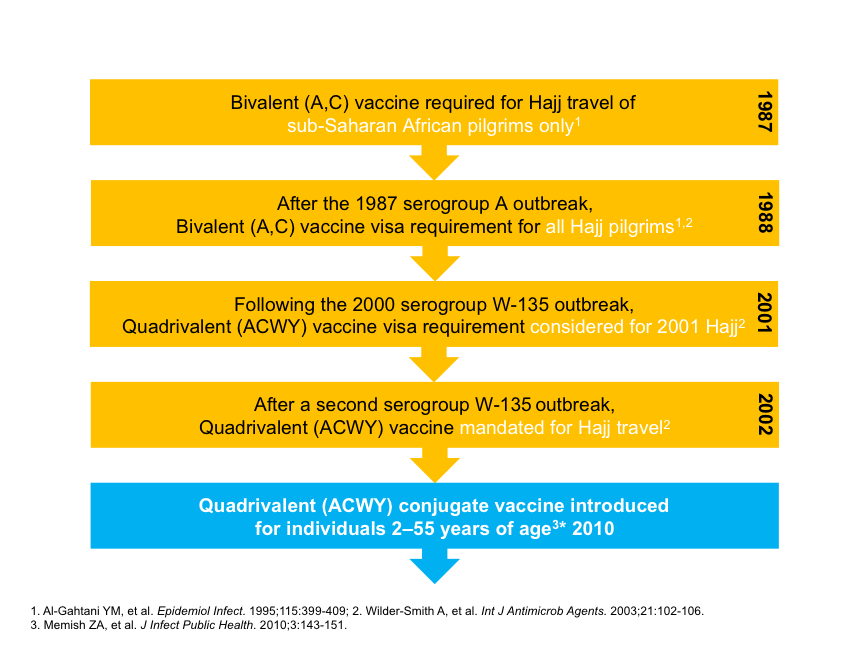
Adults and children above 2 years old arriving for the Hajj pilgrimage (or for seasonal work in the Hajj area) are required to produce a vaccination certificate of the quadrivalent vaccine against IMD, which has been issued not more than three years and no less than 10 days ago prior to arrival in Saudi Arabia.
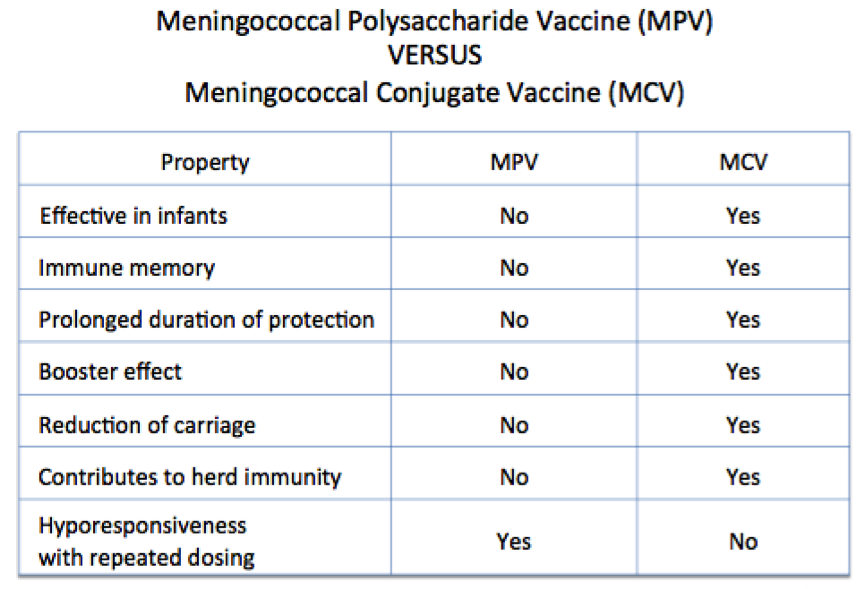
There are two types of quadrivalent meningococcal (MenACWY) vaccines available. The Meningococcal Polysaccharide Vaccine (MPV) and the more recent and more contemporary and effective Meningococcal Conjugate Vaccine (MCV).
The vaccine of choice is the MCV, which can be administered to children below 2 years, and confers immune memory, reduce carriage, and contributes to herd immunity.
The MPV can only be used for children above 2 years, does not confer immune memory, does not reduce nasopharyngeal carriage, and does not contribute to herd immunity.
There is now an increasing emergence of replacement serogroups, namely MenB in countries eliminating MenACWY with the quadrivalent vaccine in their national immunisation programmes, and serogroup X in the African meningitis belt.
Global and national surveillance of IMD needs to be strictly continued to ensure early detection and prediction of changing disease epidemiology as has happened in the past 36 years and implement early prevention and control strategies.
Currently available MenB vaccines and novel pentavalent (MenABCWY, MenACWXY) vaccines could be considered for further protection against other serogroups of IMD.
Seasonal Influenza
Acute respiratory infections (ARI) were the most frequent diagnosis among sick pilgrims during the Hajj seasons. About 62 to 71 per cent of pilgrims reported respiratory symptoms. The prevalence of influenza viruses varied from 4.3 to 14 per cent.
A meta-analysis of 18 studies with a total sample size of 62,431 estimated that the overall prevalence of influenza viruses was 5.9 per cent. The prevalence of viruses increased from 7.4 per cent in pre-Hajj samples to 45.4 per cent in post-Hajj ones.
The nature of Hajj rituals and the persistent state of overcrowding enhances the transmission of ARIs and the exportation of pathogens by the returning pilgrim.
Some 29 out of 42 studies reported on the uptake and effectiveness of influenza vaccine among pilgrims, and five studies both influenza and non-influenza vaccines. The coverage of seasonal influenza vaccine ranged from 0.7 to 100 per cent.
The uptake was highest in the elder persons and those with comorbidities. The influenza vaccine effectiveness (VE) varied across the different studies.
Pooled estimates from six studies showed that the influenza vaccine was significantly effective against laboratory-proven influenza among Hajj pilgrims (risk ratio 0.56; 95% CI 0.41-0.75; p <0.001).
The Saudi health ministry has recommended the influenza vaccine since 2005 for all pilgrims, particularly for those at increased risk, which includes the elderly and those with comorbidities and immunosuppression.
The Saudi health ministry’s current Hajj regulations and guidelines mandate obtaining influenza vaccinations for domestic pilgrims, while it is only recommended for international pilgrims.
The seasonal influenza vaccine is highly recommended for prospective Hajj pilgrims at least two weeks before leaving their country of origin. The most recent quadrivalent influenza vaccine as advised by the World Health Organization (WHO) should be used.
Invasive Pneumococcal Disease (IPD)
Pneumonia is the leading cause of hospital admissions during Hajj, contributing 20 to 39 per cent. The most common organism isolated was Streptococcus pneumoniae (50 per cent).
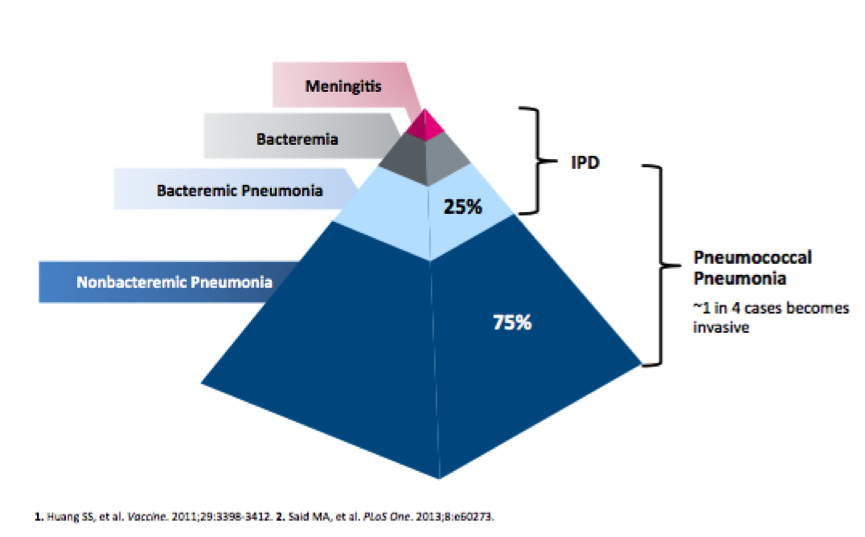
Unlike children, pneumococcal pneumonia constitutes the vast majority of disease in adults. Meta-analysis of community-acquired pneumonia (CAP) studies reporting pneumococcal detection estimated that 25 per cent of pneumococcal pneumonia cases are bacteremic.
Pneumococcal pneumonia may cause higher rates of complications and deaths in older people aged 65 years and above, especially those with chronic medical conditions.
Approximately 7 to 37 per cent of pilgrims are 65 years of age or older. Chronic medical conditions among pilgrims include diabetes mellitus (20 to 40 per cent), obesity (30 per cent), bronchial asthma (10 per cent), chronic obstructive pulmonary disease (10 per cent), and tobacco smoking (10 per cent).
At the global level, two vaccines are currently available for pneumococcal vaccination in adults. There is the 23-valent pneumococcal polysaccharide vaccine (PPV23) and the pneumococcal 13-valent conjugate vaccine (PCV13).
Even though the pneumococcal vaccine has not been mandated for Hajj pilgrims due to the lack of available data, it is very important for the high-risk pilgrims to receive the pneumococcal vaccine. The current uptake is low, at 5 per cent.
The pneumococcal conjugate vaccine (PCV13) is the preferred choice for the pneumococcal naïve pilgrim. Those who have been vaccinated with the PPV23, can receive the PCV13 one year after the most recent dose of PPV23.
Covid-19 Pandemic
Saudi Arabia suspended the Umrah (minor pilgrimage) for international pilgrims in February 2020, which was followed by a full lockdown of the Grand Mosque one month later. The Hajj in late July 2020 was performed by 1,000 pilgrims, compared to the usual two million.
In July 2021, citizens and residents in Saudi Arabia were allowed to perform the Hajj, conditional upon receiving two doses of the Covid-19 vaccine. The vaccine has been available in Saudi Arabia since December 2020.
Almost one million pilgrims performed the Hajj in early July 2022. About 85 per cent of them were international pilgrims. The Saudi health ministry has mandated all Hajj pilgrims to be between 18 and 65 years of age, and to have at least two doses of Covid-19 vaccination.
Other Vaccines For Hajj
Some of the vaccines you had when you were younger may require boosters. Do check your immunisation history for conditions such as:
- Diptheria, tetanus, and acellular pertussis. You may require a Tdap booster.
- With the recent resurgence of measles and rubella, check that you have had two doses of MMR or a previous history of natural measles.
- Food and water-borne infections, e.g. Hepatitis A and typhoid fever.
Pilgrims From Select Countries
The Saudi health ministry has additional vaccination requirements for Hajj pilgrims entering from certain countries. All travellers arriving from countries known to be infected with yellow fever must present a valid yellow fever vaccination certificate. The list of countries can be found here.
All travelers arriving from countries with circulating polio virus or from countries at high risk of re-importation of polio virus, regardless of age and vaccination status, should receive one dose of polio vaccine.
Conclusion
The Hajj season is an annual mass gathering of about two million pilgrims. The Saudi Hajj ministry has already planned for the 2030 season, which will see up to six million pilgrims performing the Hajj.
Large outbreaks of communicable diseases are a real public health threat during the Hajj period. A stricter and comprehensive vaccination policy of all pilgrims, especially high-risk elder persons and those with comorbidities against influenza and invasive pneumococcal disease should be seriously considered, apart from the mandatory vaccination against invasive meningococcal disease.
Continuous surveillance of respiratory pathogens must be prioritised to ensure early detection and immediate intervention to prevent potential outbreaks.
Dr Husna Musa is a paediatrician and lecturer at the Department of Paediatrics, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia. Dr Musa Mohd Nordin is a consultant paediatrician and neonatologist at KPJ Damansara Specialist Hospital.
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.



