

The scientific evidence accumulated after more than a year of the Covid-19 pandemic points conclusively to the predominant long-range (more than five feet) airborne nature of its transmission.
To date, this important feature of the infection has only received cursory attention from authorities and policymakers worldwide, and more so by the general public.
Therefore, our existing pandemic management measures, focusing solely on droplet and fomite transmission, might be extensive, but sub-optimal.
On April 15, 2021, The Lancet medical journal published an article entitled “Ten Scientific Reasons in Support of the Airborne Transmission of SARS-CoV-2”. Around the same time, two other medical journals, namely The British Medical Journal (BMJ) and Journal of the American Medical Association (JAMA) also published articles in a similar vein.
The following is a simplified summary of the scientific reasons and facts listed by Professor Greenhalgh and her colleagues in The Lancet article, which strongly points towards the important (if not predominant) role of airborne nature of Covid-19 transmission, backed by accumulated scientific evidence.
The first such factor is the presence of super spreaders and super spreading events — whereby one infected individual becomes responsible for infecting a large proportion of those present in the same premise, but not necessary within five feet from the infected. Only the airborne nature of transmission can adequately explain the frequency of such infections in the Covid-19 pandemic.
Secondly, in a New Zealand study by Eichler and team, the researchers, while methodologically combining genomic sequence analysis and epidemiologic investigation, have proven the possibility of airborne transmission between people in adjacent quarantine hotel rooms, who were never in direct contact with each other.
Thirdly, according to the latest estimates, asymptomatic individuals are responsible for transmitting close to 60 per cent of all infections. Asymptomatic individuals are not sneezing or coughing much.
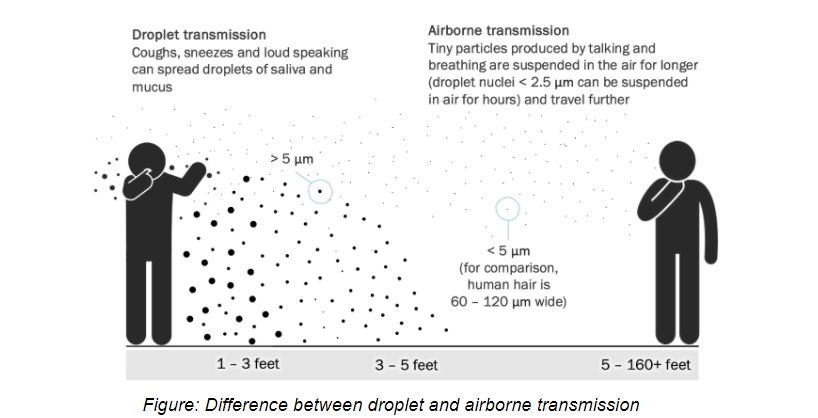
Therefore, it is pretty difficult to explain such a distribution of infections unless we consider the role of airborne transmission. The smallest particles (droplet nuclei more than five μm) laden with the viable virus and capable of travelling long distances in the air are found to be emitted even while low voice talking or just breathing.
Fourthly, it is well established that the risk of Covid-19 transmission is significantly lower outdoors than indoors, and in well-ventilated versus poorly ventilated indoor settings, consistent with airborne transmission.
Fifth, the Covid-19 spreads were reported in hospital environments with protective measures explicitly designed to address large droplet concerns, but not the possibility of airborne transmission.
Sixthly, scientists have detected viable Covid-19 viruses in the air samples in laboratory conditions for up to three hours. However, detecting airborne viruses outside of laboratory settings is challenging, due to mechanical damage during sampling. Authors also stress that other infections such as measles and tuberculosis, whose primary airborne route of transmission is undeniable by now, “have never been cultivated from room air”.
Seventhly, scientists at Uppsala University Hospital, Sweden, have detected SARS-CoV-2 N and E genes inside the ventilation HEPA filters, located too far outside the range of large droplet transmissions. In the said Swedish study, the researchers could extract only genetic material rather than viable viruses, due to sampling challenges described earlier.
Eighthly, another scientific experiment supporting tje airborne mode of SARS-CoV-2 transmission has been conducted in the Netherlands. Jasmin Kutter and her colleagues have demonstrated transmission of SARS-CoV-2 to two of four indirect recipient ferrets and SARS-CoV to all fourm while eliminating the possibility of direct transmission between animal enclosures.
Ninthly, to the best of Professor Greenhalgh and her other colleagues’ knowledge, no study so far “has provided strong or consistent evidence to refute the hypothesis of airborne SARS-CoV-2 transmission”, while empirical evidence suggesting otherwise is piling up.
Tenthly, the authors have demonstrated the inconclusiveness of arguments that have been put forward in favour of predominant close-contact (large droplets and fomites) Covid-19 transmission. A higher risk of close-contact infection does not prove that the Covid-19 virus predominantly travels in droplets, and does not contradict the hypothesis about its airborne transmission.
How convincing does all of this sound? It is compelling enough that even the World Health Organization (WHO), on April 30, 2021, updated the English version of its Q&A section with regards to Covid-19 spread between people by adding a paragraph that underscores the possibility of long-range virus transmission in poorly ventilated and/or crowded indoor settings.
Note that previously the WHO and the Centers for Disease Control and Prevention (CDC), while did not outright deny the possibility of large-distance airborne nature of Covid-19 transmission, solely emphasised the close-contact or short-range modes of transmission (large droplets and fomites).
The other two articles in BMJ and JAMA also echo the proposition about SARS-CoV-2 likely having a predominant airborne transmission route. They also discuss the implications of this scientific finding for effective non-pharmaceutical intervention.
Wearing masks, physical distancing, limiting indoor occupancy and crowded outdoor activities remain relevant measures to curb infection, either from direct contact with surfaces or droplets, or from inhaling droplet nuclei. However, when we consider accumulated scientific evidence about airborne transmission, a few concerns immediately arise about the sufficiency of the existing efforts.
Firstly, the engineering control of indoor air quality — ventilation and filtration — in work environments, educational institutions, shopping malls, recreational public spaces, and even our homes, become essential. It is pertinent to ask about the current conditions of the ventilation and filtration systems in these spaces. Except for hospitals, they are probably be set for the bare minimum, and will not be designed for effective infection control.
The airborne nature of the Covid-19 virus calls for a thorough revision and upgrade of ventilation and filtration standards and systems nationwide. Public spaces deserve immediate attention.
As an immediate solution, increasing the humidity level in public spaces would significantly reduce the travel distance of droplet nuclei laden with the virus. Additionally, IoT devices measuring CO2 concentrations can be placed strategically to detect dangerous levels. In public spaces, it is also possible to think of gaseous disinfectants (similar to the one sprayed before airline takeoff) released periodically throughout the day.
In the long run, authorities must make ventilation and filtration standards, required to combat airborne infections effectively, part of development standards. Allen and Ibrahim discuss at length the required targets for ventilation and filtration in various settings grounded in the basics of exposure science in the aforementioned JAMA article published on April 16, 2021.
Also, reducing taxes for companies involved in manufacturing, installing, and maintaining high-efficiency ventilation and filtration systems will increase general public access nationwide.
The revision and upgrading of ventilation and air conditioning systems might seem a daunting task, and comes with many fixed costs. However, the tremendous savings and other benefits that can be realised from improved public health and reduced sick leave for other respiratory viruses nationwide will far outweigh the costs.
Additionally, the use of smart systems tracing the occupancy or CO2 concentration may significantly reduce the costs of operating such systems.
Such indoor air control system overhauls would also increase our resilience and reduce costs associated with possible future pandemics and air quality-related disasters. But it is also crucially important now, especially when we do not know how long more we will have to combat Covid-19 and its possible variants.
The second major concern is the quality of masks used — high filtration efficiency and a tight fit are crucial for adequate protection against inhaling aerosols.
The airborne nature of the Covid-19 virus also requires tailoring intervention strategies and tightening SOPs for locations where masks are not worn all the time, for example, in restaurants. It is mandatory for waiters to wear high-efficiency masks and for patrons to wear masks at all times except eating.
The accumulated empirical evidence of airborne Covid-19 viruses discussed here should not only make governments and health officials heed the science and re-focus their efforts, but should also make the general public more cautious and vigilant to comply with SOPs. Don’t let your guard down. This virus, SARS-CoV-2, might be more subtle and ubiquitous than we think it is.
Rais Hussin and Margarita Peredaryenko are part of the research team at EMIR Research, an independent think tank focused on strategic policy recommendations based on rigorous research.
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.



