

Two local doctors have proposed the idea of administering the Sinovac vaccine in Malaysian children aged 3 to 17 years old.
This is based on the approval by the Chinese regulators of Sinovac Biotech’s inactivated Covid-19 vaccine, Coronavac, for emergency use in children between 3 and 17 years of age.
I am much concerned that they are basing their opinions on a press statement released to the Chinese state media, instead of data from a publication in a peer-reviewed scientific journal.
This is not how scientists or national regulators judge a vaccine for public use, especially for a young age group. The interim vaccine data must be meticulously verified and validated.
It is simply due to this lack of transparency that none of the Chinese vaccines have been sanctioned for emergency use by the US Food and Drug Administration (FDA) or the European Medicines Agency (EMA).
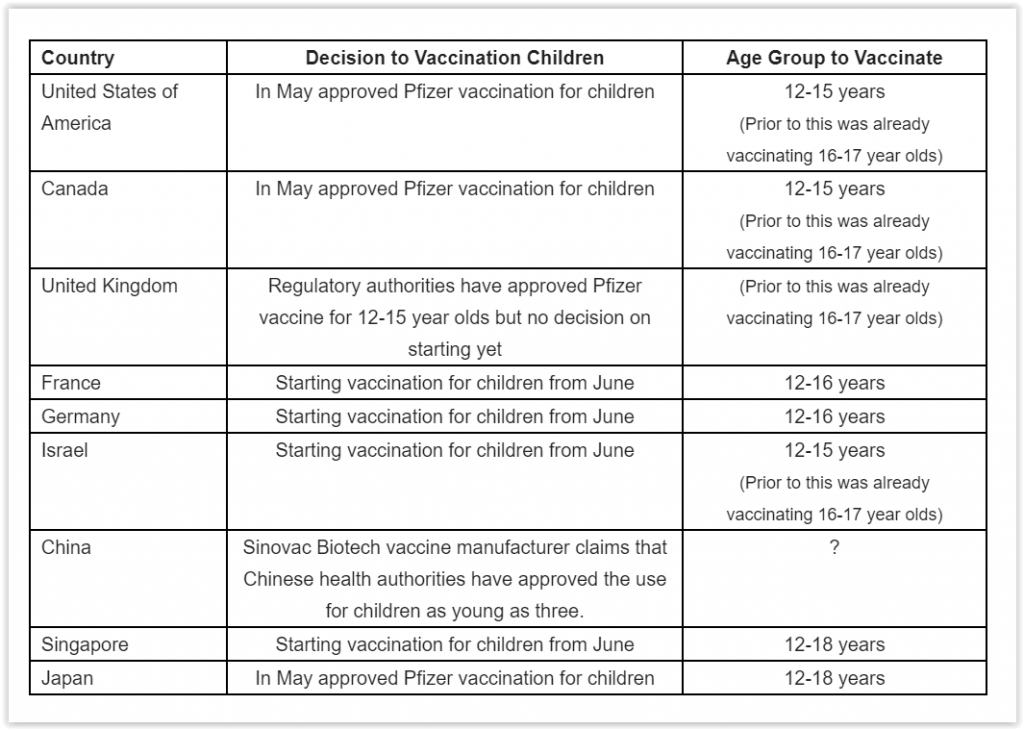
Even the World Health Organization (WHO) has only approved the Sinovac vaccines for emergency use only in those aged 18 years and older.
The regulators in the US, Britain, Singapore and the European Union have approved the Pfizer-BioNTech vaccine for those as young as 12 years old.
This followed the interrogation of the interim analysis of the Pfizer-BioNTech vaccine used in 12-to-15-year-olds, which showed a favourable safety profile, produced a greater immune response than in young adults, and was highly effective against Covid-19.
The other reason to treat with caution the proposition of the two local doctors is their lack of grasp of the epidemiology of Covid-19 in the pediatric age group.
Up until June 1, 2021, there have been 82,341 reported cases in children under 18 years old. This is 14.2 per cent of the total number of cases (579,462 cases).
There were 15 deaths among children aged below 18 years, which is 0.52 per cent of the 2,867 deaths reported as of June 1.
The case fatality rate (CFR) among the pediatric age group was 0.02 per cent as compared to 0.57 per cent in the adult population, which is 29 times more deadly.
Children below 18 years comprise 29 per cent of the total population, i.e. 9.3 million. The risk of Covid-19 deaths in children less than 18 years is approximately 2 per million.
Nine (60 per cent) of the deaths were associated with comorbidities and it is unfortunate that six (40 per cent) of the deaths occurred in otherwise healthy children. Even this, I suspect, might be even lower if we had access to their medical records and autopsy details.
This contrasts with the experience in the US. Utilising approximately 50 per cent of the US health insurance data from FAIR Health, the team at Johns Hopkins University showed that all of the children who died from Covid-19 had a pre-existing comorbidity. This would make a case for vaccinating a child with an underlying illness.
Within the pressing context of a restricted global supply of vaccines, many pediatricians have pleaded for the judicious and priority utilisation of precious Covid-19 vaccines.
In an opinion piece in the Washington Post, Richard Malley (Harvard University) and Adam Finn (University of Bristol) wrote, “Speaking as pediatricians who are also vaccine researchers, we say: Please don’t make a priority of immunizing healthy children 2 to 11 years old against the coronavirus.”
The May 2021 editorial in the BMJ echoed a similar sentiment: “Covid-19 severity in children under the age of 12 is similar to that of influenza, and as health resources are stretched thin even in high income countries vaccinating children is unlikely to be a priority.”
I have shown that the risk of a healthy American child and a healthy Malaysian child dying from Covid-19 is zero and 0.6 per million respectively.
I would therefore reiterate that there is no compelling case for Covid-19 vaccines in healthy children as proposed by the two local doctors.
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.



