

In the past couple of weeks, there have been many articles and comments written about this issue after the president of Association of Private Hospitals (APHM) made a request to Vaccine Minister Khairy Jamaluddin that private hospitals be allowed to procure vaccines on their own to complement the effort of the government in vaccination to achieve faster “herd immunity”.
According to Dr Kuljit Singh, there are expatriates and those with diplomatic immunity that want to travel and want to be vaccinated earlier and also companies may choose to fund inoculation of their employees. He further added that it will give opportunity to people who require the vaccine earlier to be inoculated due to their increased interaction with others or because of business, work or religion that require them to travel.
The member hospitals of APHM and other private hospitals have agreed not to impose any surcharge on the vaccine and that vaccines will be administered at the cost of procurement.
According to the Special Committee for Ensuring Access to Covid-19 Vaccine Supply (JKJAV), the National Covid-19 Vaccination Programme involves 3 phases, in Phase 1 from 24 February to April involving 500,000 public and private health care personnel and other frontliners.
Phase 2 from April to August will involve some 9.4 million people including reminder of health care workers, essential services, and from those aged 65 and above, as well as high-risk groups and people with disabilities. Phase 3 will start from May this year till February 2021, involving both Malaysians and non-Malaysians covering those aged 18 and above, involving another 13.7 million people.
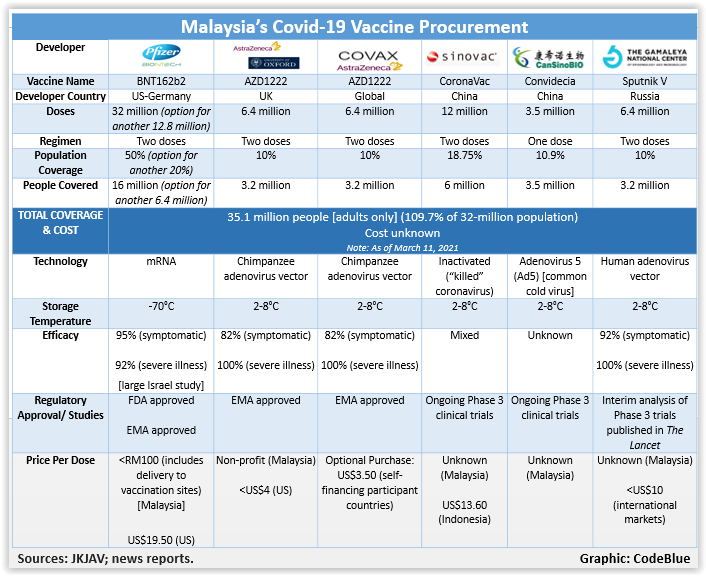
Malaysia has acquired five different types of vaccines for a total of 66.7 million doses covering 109.65 per cent of those in the country.
There is some strong support for the above view for a private market. People who are at the back of the national vaccine programme queue who want to pay should be allowed to do so.
There is also the view that after health staff, other frontliners and vulnerable that have been vaccinated, there can be a private market for it.
Another view is that some people are more comfortable with their private health care provider and therefore they should be allowed to choose and pay for their vaccination as in other national vaccination programme.
Some also argue that they do not have trust and faith in the priority list of the national vaccination rollout, and therefore, the national vaccination programme should be opened up. This is will also open up slots to others and removed from the national list and thus reduce waiting time. The participation of the private sector can expedite the vaccination rollout and therefore hasten the health and economic recovery of the country.
But there are many who are not in favour of this private market. The main argument against it, is the inequity issue. If the private market is allowed and with limited supply of the vaccine, then those who are health staff, other front-liners and vulnerable may not be vaccinated.
This “queue jumping”, or commercialisation according to some critics of the private market, will further widen the access gap to this vaccination between the haves and have-nots. It is even more important for the poor and vulnerable to be vaccinated earlier as they live and work in crowded and less than satisfactory conditions. Further, they are more prone to be infected than the rich and privileged.
The Malaysian health care system is a dual system with the private sector contributing a significant proportion in terms of its financing, facilities (clinics and beds), delivery of services (especially in the urban areas) and human resources (specialists, nurses and other health professionals).
In the National Immunisation Programme (NIP), both the public and private sectors are involved in procuring and administering the vaccines, but generally they are for a specific age group/ sex. In the NIP, vaccinations are provided free-of-charge at all public health facilities, while those in the private health facilities pay for them.
But for this Covid-19 vaccine, it involves nearly the whole population, those who are above aged 18 and eligible to be vaccinated and the government has committed to pay for all these vaccinations. They will be carried out in government health facilities and other public facilities, private clinics and hospitals.
Private GPs who wish to be vaccinators can register with ProtectHealth Corporation, a company owned by the Ministry of Health. They will be involved in the 2nd and 3rd phase of the National Covid-19 Vaccination Programme.
Private hospitals have also been included as vaccinators, as announced by Sunway Medical Centre and Subang Jaya Medical Centre. They cater mostly to private health care providers in phase 1 of the programme.
The Vaccine Minister announced, in a reply to former Prime Minister Najib Razak, that if private parties are able to purchase vaccines from the manufacturers for those vaccines that have been approved by the National Pharmaceutical Regulatory Agency (NPRA), they are welcomed to do so.
This is a departure from the previous policy that the government will consider opening up the vaccine market after 80 per cent of the population have received the vaccination and reach herd immunity. This is also a departure from the stance of APHM that they be allowed to purchase vaccines that are not procured by the government.
I am not surprised that the government is willing to open up the market as there is continued pressure from private hospitals (many are owned by GLCs such as IHH, KPJ and Sime Darby), advocacy by some medical personnel, and other public figures. The reasons cited have already been mentioned above.
Some want the ability to choose the type of vaccine and when to be vaccinated as they are paying from their own pocket. What is surprising to me is the sudden shift in this policy comes so early as we have not even completed phase 1 of the vaccination programme.
We will be joining countries like Indonesia and India that have opened up their vaccination programmes to the private market as their public health system is unable to cope. For us, we are opening up to the private market for other reasons. This is not surprising to many as in Malaysia, we have always have “choices” whether in education, health, or even paying tolls!
- This is the personal opinion of the writer or publication and does not necessarily represent the views of CodeBlue.


