
I refer to the letter titled, ‘There’s no basis for banning female circumcision’ written by Rafidah Hanim Mokhtar and Nur Saadah Khair.
It is shocking that they and Wafiq, the International Women’s Alliance for Family Institution and Quality Education, are defending female genital cutting. It is alarming that as medical professionals, rather than depending on science, they place religious practices at the centre of their argument.
Despite their demand for an objective analysis of female genital cutting (FGC) backed by reliable and validated data, they have conveniently ignored the fact that there is no scientific data or medical evidence whatsoever which justifies the need or benefits for performing this procedure.
Until recently, it is a practice that barely raised an eyebrow even among the media, human rights and women’s rights activists in the country. It is a fact for many Muslims in Malaysia that FGC, also euphemistically termed as female circumcision, is routinely carried out on infants and girls.
Everyday, this procedure is being done. But just because everybody does it, does not make it right.
The euphemistic term of female circumcision and the above response has been used repeatedly to make it sound better and justify the practice.
One of the common responses to the practice of female genital cutting in Malaysia is that we don’t do it the way it is done in Africa. So, it is acceptable to do it.
Let us be clear, any harmful procedure which is carried out on the female genitalia for non-medical purposes, whether minor or major, is female genital mutilation. This is also known as female genital cutting.
Female circumcision is female genital cutting.
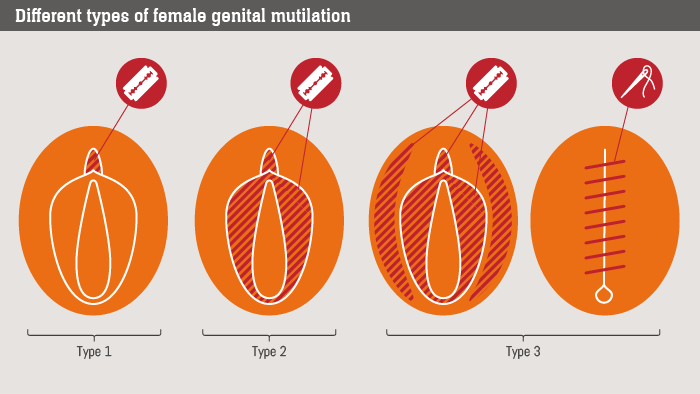
The World Health Organization (WHO) has four classifications for FGC:
- Type 1 is clitoridectomy – partial or total removal of the clitoris and, in very rare cases, only the prepuce or clitoral hood (the fold of skin surrounding the clitoris).
- Type 2 is excision: partial or total removal of the clitoris and the labia minora, with or without excision of the labia majora or “the lips” which surround the vagina.
- Type 3 is infibulation: narrowing of the vaginal opening through the creation of a covering seal. The seal is formed by cutting and repositioning the inner, or outer, labia, with or without removal of the clitoris.
- Type 4 includes all other harmful procedures to the female genitalia for non-medical purposes. This includes the procedure of pricking, piercing, incising, scraping and cauterising the genital area.
Malaysia has Type 1, 2 and 4. We do not have Type 3 which is the practice of infibulation, a form of FGM which has traumatised, scarred and damaged the lives of thousands of girls and women in Africa and some parts of Asia.
WHO also concluded that in comparison to the clear, demonstrable benefits for male circumcision ranging from improved hygiene and prevention of sexually transmitted diseases, there are absolutely no medical benefits from female genital cutting.
The following might sound familiar:
- “You know, the blade used in those old Gillette shavers which you can buy at the convenience store? The blade is lightly run across the clitoris and the labia”
- “Just a pinprick aja. A hole was made into the clitoral hood.”
- “A small bit of the labia or the clitoral hood was sliced off.”
- “I remove a centimetre of the clitoris.”
The first and last quotes were from a traditional practitioner, while the rest are some of the common descriptions given by women and girls who have been subjected to the procedure which was described to them by the mothers. They are some of the usual options offered by private hospitals and clinics. The fees range from RM 50 to RM 400.
Based on descriptions of the procedure as implemented around the country, three out of the four forms of female genital cutting are practised in Malaysia.
A ministry of health circular actually prohibits the practice of female circumcision in all public health facilities. Rather than medicalising and regulating the practice, MOH should extend that prohibition to all healthcare facilities, private and public.
Despite all of this, mothers continue to insist on having their infant daughters’ genitals cut. Why?
The University of Malaya study on the status of female circumcision in Malaysia cited by Rafidah Hanim and Nur Saadah indicated the following findings:
- More than 90% of Malay Muslim female respondents were circumcised.
- None of the non-Malay female respondents were circumcised.
- More than 93% of women also circumcised their daughters.
- The primary reasons for female circumcision were cited as it being a religious obligation, personal hygiene, cultural practice and to control the girl’s sexual desire.
In 2006, Al Azhar University declared female circumcision as un-Islamic.
Since then several Muslim majority countries have banned the practice including Egypt and Indonesia (despite the ban, the cutting of girls persists in many rural areas). In 2012, the UN General Assembly’s human rights committee adopted a resolution which declared female genital cutting to be a harmful practice and a serious threat to the psychological, sexual and reproductive health of women and girls.
The National Fatwa Council in 2009 made the practice obligatory (wajib) for girls (http://e-smaf.islam.gov.my/e-smaf/fatwa/fatwa/find/pr/15253). Yet, their rationale couldn’t even find the necessary references in the Quran and had to utilise arguments from a different mazhab (Maliki).
In comparison, slavery is not only mentioned in the Quran, but it is also provided for as an accepted practice in certain circumstances. Yet, we don’t accept or practice slavery today. We condemn it. Last I checked, none of the Muslims I know owned any slaves.
Contrary to what is being claimed, female circumcision isn’t required under Islam. There are no medical benefits from the procedure. There is also no evidence that female circumcision does anything to control sexual desire (unless because of the circumcision, the sex act is so traumatic that it would be too painful or impossible).
If there is no medical benefit, no religious obligation, or any benefit whatsoever to performing female circumcision, then why do it?
Rather than medicalising the practice, we should instead be prohibiting and criminalising the act of female circumcision to protect our infant daughters and girls from harm. No ifs, buts or caveats.

Azrul Mohd Khalib is the founder and CEO of Galen Centre for Health and Social Policy.





